Bridge Piercing Quick Facts
| Feature | Detail |
|---|---|
| Also Known As | Erl piercing, Earl piercing, nose bridge piercing, midbrow piercing |
| Piercing Type | Surface piercing |
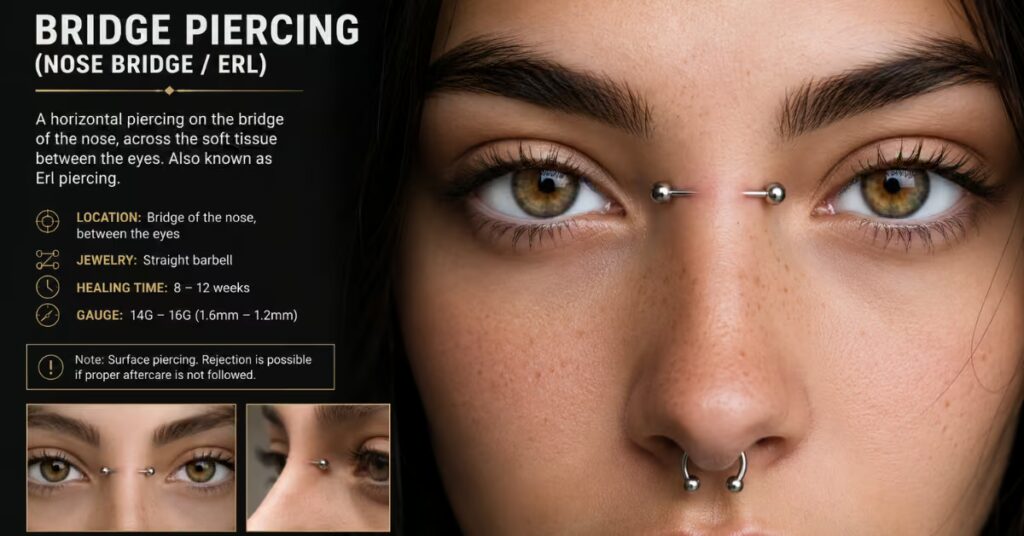
| Location | Horizontally through the skin on the upper nose bridge, between the eyes |
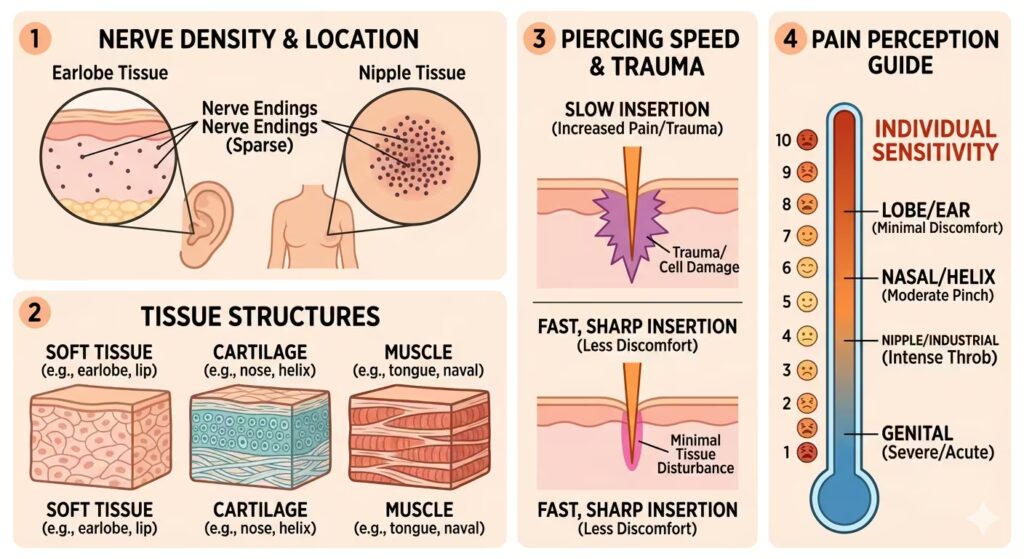
| Pain Level | Low to moderate (3–4/10) |
| Healing Time | 8–12 weeks (surface); internal healing up to 6 months |
| Average Cost | $30–$90 (jewelry not always included) |
| Standard Jewelry | Straight barbell (12 or 14 gauge) |
| Best Materials | Implant-grade titanium, niobium, implant-grade surgical steel, solid 14k+ gold |
| Rejection Risk | High — classified as a long-term temporary piercing by most professionals |
| Anatomy Dependent | Yes — not everyone qualifies |
What Is a Bridge Piercing?
A bridge piercing is a horizontal surface piercing through the thin skin on the upper nose bridge, directly between the eyes. It passes through only the epidermis and dermis — no cartilage, no bone is involved.
Unlike nostril or septum piercings, which anchor through more substantial tissue, the bridge sits in a shallow fold of skin above the nasal structure. This shallow placement is what gives it its distinctive floating barbell look — and what makes it anatomically demanding.
It’s also called an Erl piercing, named after Erl Van Aken, a client of legendary body piercer Erik Dakota. Van Aken is credited as one of the first people to wear the piercing regularly in the 1980s, and the style spread through punk and alternative subcultures through the 1990s before entering the mainstream.
Types of Bridge Piercings
- Standard Horizontal Bridge: The classic placement. A straight barbell sits horizontally across the nose bridge between the eyes. This is the most stable and most common variation.
- Vertical Bridge (Third Eye): The barbell runs vertically rather than horizontally, between the eyebrows toward the forehead. It is a dedicated surface piercing, typically done with a surface bar rather than a straight barbell.
- Double Bridge: Two horizontal barbells are placed in parallel across the nose bridge. This requires significantly more pinchable tissue than a single bridge. Many piercers will decline this if the anatomy is marginal for even a single placement.
Anatomy: The Most Important Factor
A bridge piercing is anatomy-dependent — your piercer will assess your nose bridge before agreeing to pierce. Ideal anatomy includes a defined ridge with pliable, pinchable tissue that lifts cleanly away from the bone underneath.
Candidates need an even, broad nasal bridge with sufficient tissue thickness to support the jewelry without excessive movement. If your skin sits tight against the bone with minimal tissue depth, the piercing will be under constant pressure. That tension accelerates rejection and, in cases of critically shallow tissue, can cause reduced blood supply to the underlying bone.
Some industry professionals estimate that piercers turn away 20–40% of prospective clients due to insufficient anatomy. A piercer declining you for anatomical reasons is protecting you from a fast-failing piercing and visible facial scarring.
Pain Level
The bridge area has relatively few nerve endings compared to cartilage zones. Most people describe the sensation as a sharp pinch, followed immediately by involuntary watering of the eyes — a reflexive response to anything near the eyes, not a sign of damage.
Pain subsides quickly after the needle passes through. Swelling and tenderness between the eyes are normal for the first two to three days. Over-the-counter pain relievers manage the initial discomfort for most people without difficulty.
Healing Time
A bridge piercing typically heals in 8 to 12 weeks for most people. Surface tissue heals faster than cartilage, but healing progresses from the outside in. The piercing will look and feel healed before the internal channel is fully formed.
Do not stop aftercare at the 6-week mark because it appears calm. Confirm full healing with your piercer before changing jewelry or reducing your routine. Healing timelines also depend heavily on the consistency of aftercare and how often the piercing is disturbed.
Week-by-week breakdown:
- Weeks 1–2: Swelling, tightness, and tenderness between the eyes. Some redness and a small amount of clear or white discharge are normal.
- Weeks 3–6: Swelling reduces. The healing channel begins forming. This period is when neglected aftercare causes the most damage.
- Weeks 8–12: Surface healing is complete for most people. Internal tissue may continue forming for up to 6 months.
Rejection and Migration: The Defining Risk
Bridge piercings have one of the highest rejection rates of any common piercing. Because the barbell sits in a shallow fold of skin — not anchored through cartilage or deep tissue — the body treats it as a foreign object and can push it toward the surface over time.
If your bridge piercing migrates or rejects, remove it immediately. Keeping it in longer will not save it — it only causes additional scarring. If you still want the piercing, wait until the area closes completely and returns to its normal look and feel before repiercing.
Some bridge piercings last years or even decades. Others begin migrating within months of healing. There is no reliable way to predict the outcome in advance.
Signs of rejection to watch for:
- The barbell is visibly shifting from its original placement
- Entry and exit holes appear wider than when first pierced
- Skin between the holes becomes thin, flaky, or calloused
- Persistent redness and soreness that doesn’t resolve with normal healing
Scarring
A bridge piercing that is eventually removed — whether by choice or rejection — typically leaves two small pitted marks, one at each hole. These marks sit on the face between the eyes, so they are visible.
How prominent the scarring is depends on skin type, how long the jewelry was worn, and the extent of migration at the time of removal. Removing the jewelry at the first clear signs of rejection minimizes scarring. Scars from early removal often fade significantly within a year and can become nearly invisible on some skin types. Waiting until the skin is paper-thin before removal produces more defined, permanent marks.
Jewelry
Type
A straight barbell is the correct initial jewelry for a standard horizontal bridge piercing. The barbell should sit perpendicular to the tissue for optimal stability and the lowest risk of rejection.
The initial barbell will be longer than the final fit to allow for swelling during healing. Once fully healed, your piercer will downsize the bar to a more closely fitting length. Using curved barbells or surface anchors instead of straight barbells is a common reason for elevated rejection rates — straight barbells are the correct choice for this anatomy.
For vertical bridge piercings, a surface bar is used instead.
Gauge
12 or 14 gauge is standard. A larger gauge distributes pressure over a larger surface area, which can reduce the risk of rejection for people with adequate tissue depth.
Material
The Association of Professional Piercers (APP) recommends the following materials for initial bridge piercing jewelry:
- Implant-grade titanium — The most recommended choice. Fully hypoallergenic, lightweight, and available in anodized colors. Safe for all skin types, including those with nickel sensitivity.
- Niobium — Similar properties to titanium. Safe for nearly all skin types. No medical-grade designation, but widely accepted as a safe initial material.
- Implant-grade surgical steel — Affordable and durable. Contains trace nickel; not suitable for people with nickel allergies.
- Solid 14k or 18k gold — Safe when implant-grade and solid. Avoid gold-plated pieces, which shed coating into healing tissue.
Avoid acrylic, mystery alloys, or plated jewelry for initial piercings.
Aftercare
Clean twice daily using sterile 0.9% sodium chloride solution only, with no additives. Spray directly onto both the entry and exit points. Let the solution air dry rather than wiping with cotton, which can leave fibers in the healing channel.
Do not use hydrogen peroxide, rubbing alcohol, or antibacterial soap. These damage healing tissue and increase the risk of irritation and rejection. Avoid makeup, facial cleansers with active ingredients, and skincare products near the piercing while it is healing.
Avoid touching the piercing with unwashed hands. Your hands go near your face constantly — adjusting glasses, rubbing your eyes, touching your nose. Each contact introduces bacteria and risks disturbing the healing channel. This is harder to manage for a facial piercing than for a body piercing.
Bridge Piercings and Glasses
A correctly placed bridge piercing sits above where most glasses frames rest on the nose. For most glasses wearers, a healed piercing and standard frames do not conflict.
The problem is during healing. Glasses resting against or near the piercing site create pressure, friction, and warmth — all of which accelerate rejection. Switching to contact lenses for the healing period (8–12 weeks) is the most effective solution. If contacts are not an option, bring every pair of glasses you regularly wear to your piercing appointment. Your piercer marks placement around your frames to avoid conflict.
Frames with adjustable nose pads tend to sit lower on the nose than solid plastic bridges. They offer more flexibility for accommodating a bridge piercing. After full healing, most glasses wearers manage the combination without ongoing issues — taking care when putting on and taking off frames to avoid snagging the jewelry.
Does a Bridge Piercing Make You Cross-Eyed?
No. There is no anatomical mechanism by which a surface piercing on the nose bridge affects eye convergence. <a href=”https://en.wikipedia.org/wiki/Bridge_piercing”>Wikipedia’s entry on bridge piercings</a> notes this is among the most persistent misconceptions about the piercing.
You may notice the barbell ends in your peripheral vision for the first day or two. The brain adapts quickly — the same adjustment that happens when you get new glasses frames. After that brief period, most wearers stop noticing the jewelry entirely. If the barbell ends remain distracting after the first week, the bar is likely too long for your anatomy — a fit issue, not a vision issue.
Health Conditions That Increase Risk
Certain conditions raise the risk of complications significantly:
- Uncontrolled diabetes — Slows tissue healing and raises infection susceptibility.
- Blood clotting disorders — Can cause prolonged bleeding and healing complications.
- Autoimmune conditions (e.g., lupus, rheumatoid arthritis) — Impair healing and increase infection risk.
- Nickel allergy — Avoid surgical steel; use implant-grade titanium or niobium.
- Active contact sports — Facial impact during healing poses a high risk of rejection. A snag that would be minor for a lobe or nostril piercing can cause a bridge piercing to fail.
Frequently Asked Questions
Does a bridge piercing go through bone?
No. It passes only through the soft skin tissue on the surface of the nose bridge — no cartilage and no bone are pierced.
Can I get a bridge piercing if I wear glasses every day?
Yes, with planning. Bring all your frames to your piercing appointment so placement can be marked around them. Plan to wear contacts during healing if possible. Full-time glasses wearers can maintain bridge piercings successfully with careful management.
How long does a bridge piercing last?
There is no predictable answer. Some last years. Others begin rejecting within months of healing. Because it is a surface piercing, it is generally considered semi-permanent rather than permanent.
Will I have a scar if I remove my bridge piercing?
Yes. Removal typically leaves two small marks — one at each hole. Scarring is more defined if the jewelry was worn through significant migration. Removing at the first signs of rejection produces the least visible outcome.
Is a bridge piercing the same as a third eye piercing?
No. A bridge piercing is horizontal, across the nose bridge. A third eye piercing is a vertical surface piercing placed between or above the eyebrows. They use different jewelry and carry different placement risks.
Can a bridge piercing be redone after rejection?
Yes, once the original piercing has fully closed and the skin has returned to its normal appearance and texture. Your original jewelry may still be usable for a repiercing.
How do I tell if my bridge piercing is rejecting vs. just healing?
Normal healing shows a gradual, consistent reduction in redness and tenderness over weeks. Rejection looks different: the holes widen, the barbell visibly shifts toward the surface, and the skin between the holes becomes thin or calloused. If the piercing appears to move toward the surface rather than settle, consult your piercer immediately.
Can I hide a bridge piercing?
Not fully. A clear or skin-tone retainer reduces visibility but won’t make it invisible at close range. Do not swap to a retainer during healing — early jewelry changes disrupt the forming channel.
What should I look for in a piercer for a bridge piercing?
Specifically look for a piercer with documented surface piercing experience. Ask to see healed examples of bridge piercings they have performed. Because placement precision and anatomy assessment are critical for this piercing, experience with surface work — not just general piercing — matters significantly.