The snug piercing has a reputation that precedes it: notoriously painful, anatomy-dependent, and one of the slowest cartilage piercings to settle. It is also one of the most striking ear piercings you can get, sitting horizontally through the inner ridge of the ear so both ends of the jewelry face forward.
This guide covers everything that actually matters for a snug piercing — the anatomy that decides whether you can have one at all, what the pain is really like, evidence-based healing expectations, the complications research shows are most common in cartilage piercings, and the jewelry that gives you the best chance of healing it cleanly.
What is Snug Piercing?

A snug piercing — sometimes called an anti-helix piercing — passes horizontally through the anti-helix, which is the curved inner ridge of cartilage that runs roughly parallel to the outer rim of the ear. Anatomically, it is described as a piercing through “the lower ridge of cartilage of the antihelix,” and unlike most cartilage piercings, it is pierced from one side of the ridge to the other rather than front-to-back.
That sideways orientation is what gives the snug piercing its signature look: both the entry and the exit of the bar are visible from the front of the ear, with the cartilage of the anti-helix sandwiched between them.
The piercing usually sits at the lower portion of the anti-helix, above the anti-tragus, and below the rook. Placement is dictated by the natural fold of the ridge, and a skilled piercer will typically position it through the thinnest, most defined part of the anti-helix so the jewelry appears to “cinch” the cartilage.
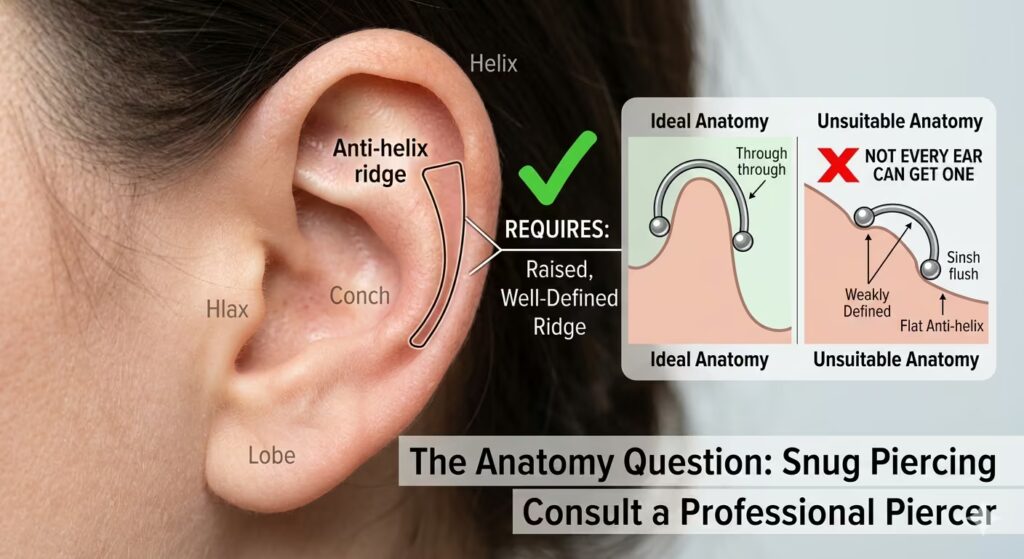
The Anatomy Question: Not Every Ear Can Get One
This is the single most important thing to understand before booking a snug piercing, and it is the reason a competent piercer will turn people away for it more often than for almost any other ear piercing.
A snug piercing requires a well-defined, raised anti-helix ridge with enough projection that a barbell can sit through it without sinking flush against the surrounding cartilage. If your anti-helix is flat, weakly defined, or too thick, a true snug piercing will not heal, and many piercers will refuse to perform it on those anatomies because the result is almost certain rejection or chronic irritation.
This isn’t an opinion problem. Studies on transcartilaginous piercings consistently show that anatomical mismatch is one of the strongest predictors of both rejection and chronic complications. A 2014 evaluation of cartilage piercing practice noted that 96% of practitioners surveyed were aware of the risk of infection, but only 4% were aware of keloid scarring and 12% of hypertrophic scarring, suggesting that screening for anatomical suitability for difficult piercings like the snug often falls short.
A reputable piercer should physically examine your ear, press the cartilage, mark a placement, and tell you honestly whether your anatomy supports it. If a piercer agrees to a snug piercing without that assessment, walk out.
If your anatomy is borderline, there is a well-recognized alternative: the faux snug piercing. This uses two separate piercings — typically a flat or helix piercing on the outer surface of the anti-helix and a conch piercing on the inner side — placed to mimic a single snug visual. Each piercing heals independently, on more forgiving tissue, and the look from the front is nearly identical. For many people, this is the only realistic way to achieve the snug aesthetic.
How Painful Is a Snug Piercing?
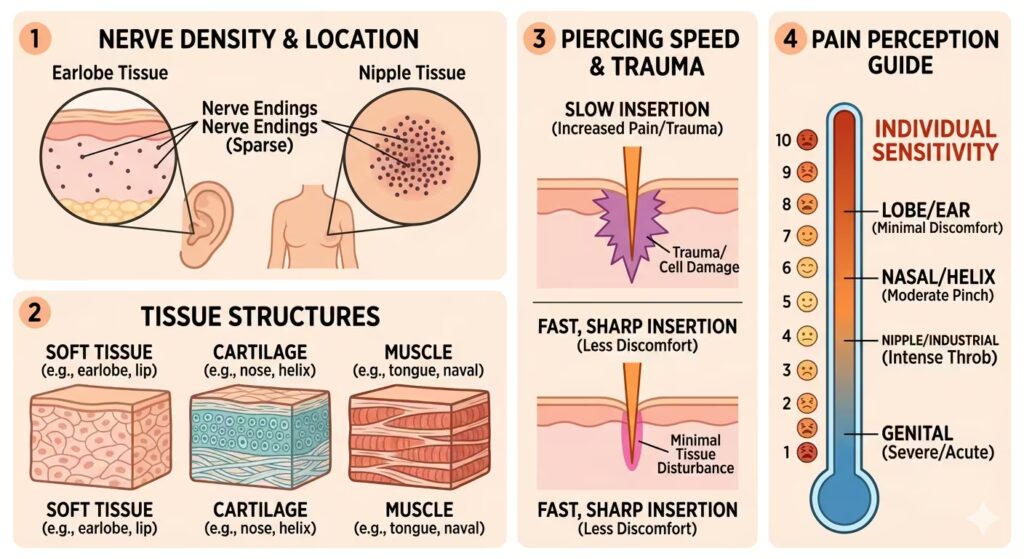
A snug piercing is widely considered the most painful cartilage piercing on the ear, and many people who have several piercings rank it as the most painful piercing they have had, full stop. The reason is mechanical, not psychological: the anti-helix cartilage is among the thickest and densest cartilage on the auricle, and the piercing passes through it horizontally — meaning the needle traverses a longer continuous channel of cartilage than something like a helix or tragus piercing.
There are typically two distinct pain moments people report:
- The pass-through. A sharp, sustained pressure as the needle works through the dense ridge. It usually takes longer than a thinner cartilage piercing because there is more tissue to cross.
- The jewelry insertion. Because the channel is curved and narrow, threading the curved barbell through can be the more uncomfortable part of the procedure for some people.
Pain is subjective, but if you are using prior cartilage piercings as a benchmark, expect a snug piercing to feel meaningfully sharper and longer than a helix or tragus. Soreness for 1–3 days afterward — especially when chewing, sleeping on that side, or using earbuds — is normal.
Snug Piercing Healing Time: Plan for a Year, Not Six Months
The honest answer on healing time is that a snug piercing behaves like one of the slowest-healing ear piercings. The anti-helix piercing has a limited blood supply compared to soft tissue, the piercing channel is long, and the area is constantly disturbed by sleeping, headphones, hats, and even facial expressions that flex the ear.
A practical timeline:
- 0–6 weeks: Acute healing phase. Swelling peaks around days 3–7, then slowly subsides. The piercing is most vulnerable to infection during this window.
- 2–4 months: Outer healing — the visible entry and exit holes look settled, but the channel inside is still epithelializing.
- 6–9 months: Most snugs are functionally healed at this point, but the channel is still maturing.
- 9–12+ months: Full healing, including the channel hardening enough to safely change jewelry without trauma. Some people legitimately need 12–18 months.
Do not let how the piercing looks on the outside trick you. Cartilage piercings can appear healed externally for months while the internal tissue remains raw. Changing jewelry too early — even at month 4, when many people get impatient — is one of the most common causes of irritation bumps, prolonged healing, and rejection.
Snug Piercing Aftercare That Actually Works
The Association of Professional Piercers (APP), the leading professional standards body for piercers, gives specific, evidence-based aftercare guidance that should anchor your routine. Sterile saline labeled for wound wash is the recommended cleaning solution, containing only 0.9% sodium chloride as the sole ingredient.
Mixing your own sea salt solution is no longer recommended by the APP, as homemade mixtures are often far too salty and can over-dry and irritate the piercing. Contact lens saline, eye drops, and nasal sprays are not appropriate substitutes — their formulations are different.
A clean, evidence-aligned routine for a snug:
- Wash your hands thoroughly before any contact with the piercing.
- Saline rinse 1–2 times daily during the active healing phase. Saturate clean, non-woven gauze with sterile saline and hold it against the piercing for 1–3 minutes, then rinse briefly with clean water and pat dry with disposable paper towels, not a towel (towels harbor bacteria and can snag the bar).
- Do not rotate the jewelry. This was old advice and is now strongly discouraged. Rotating drags scabs and bacteria into the channel, re-injuring healing tissue.
- Sleep on the opposite side for the entire healing period. A travel pillow with the hole positioned over the ear is genuinely useful and not overkill — pressure on a fresh, snug pillow for hours every night is one of the leading causes of migraines and irritation bumps.
- Skip earbuds and over-ear headphones for the first several months. Both press directly against the anti-helix.
- Avoid swimming pools, hot tubs, lakes, and oceans for at least the first 8–12 weeks. A documented outbreak of post-piercing cartilage infections found that contaminated aftercare solution and piercing location were primary risk factors, with Pseudomonas aeruginosa being the bacterial culprit in 60% of hospitalized cases. Pseudomonas thrives in standing water.
- Keep hair products, makeup, and fragrance off the area. Hairspray drift alone can irritate a healing snug piercing for days.
- Attend your downsize appointment. Once the initial swelling has gone down (usually 6–12 weeks), your piercer should replace the long initial bar with a shorter one. Skipping this step leaves a bar long enough to catch on hair, pillows, and clothing — which is itself a common cause of rejection.
Snug Piercing Risks and Complications
Cartilage piercings carry a higher complication rate than soft-tissue piercings, and the snug piercing — because of where it sits and how long it takes to heal — sits at the harder end of that spectrum. The published research is worth knowing.
A large survey study published in The Laryngoscope found that cartilage piercings carried a complication rate of 40.2% compared with 25.4% for lobule piercings, and when controlling for other variables, cartilage piercings had odds of any complication 2.2 times higher than lobule piercings. The same dataset found that infection rates were significantly more common in the cartilage group at 30.3% compared with 23.8% in lobule piercings.
Earlier landmark research reported similar numbers: a 1998 study of 1,200 pierced sites found that 35% of nurses with ear piercings reported a complication, with 30% of pierced sites developing complications, including minor infection (77%), allergic reaction (43%), keloid (2.5%), and traumatic tear (2.5%).
The specific risks worth understanding for a snug:
Perichondritis (Cartilage Infection)
This is the complication piercers and ENTs take most seriously, and it is far more dangerous than a typical “infected piercing.” Perichondritis is an infection of the connective tissue surrounding cartilage, and, untreated, it can destroy the cartilage itself.
A systematic review of cartilage-piercing infections concluded that transcartilaginous post-piercing infection may lead to ear deformity and hospitalization, with Pseudomonas the most common bacterial pathogen, and that initial antibiotic selection should be optimized accordingly. A separate clinical review noted that when perichondritis becomes associated with subperichondral abscess and cartilage loss, it becomes difficult to treat and can cause cosmetic deformities, including “cauliflower ear,” with little likelihood of successful plastic reconstruction.
The signs to watch for go beyond ordinary irritation: spreading redness across the ear (not just at the piercing), the ear becoming hot to the touch, increasing throbbing pain rather than gradual improvement, fever, and any green or foul-smelling discharge.
These are emergency-room signs, not “wait and see” signs. The standard antibiotics primary care doctors prescribe for skin infections often do not cover Pseudomonas — if you suspect perichondritis, mention the bacterium by name and ask for a referral to ENT if needed.
Rejection and Migration
The snug has one of the highest rejection rates among ear piercings, and the reason is mechanical. The anti-helix is under near-constant micro-stress from sleeping, ear movement, and external pressure, and over time, the body can decide that the foreign object isn’t worth tolerating. Jewelry slowly migrates toward the surface, the tissue covering it thins, and eventually, the bar is held in by almost nothing.
Early signs of migration to watch for: the snug piercing visibly sitting closer to the surface than it did originally, the cartilage covering the bar appearing thinner or developing a V-shape rather than a smooth C-shape at the edges, and recurring irritation bumps that scab, peel, and return in roughly the same spot. If any of these appear, see your piercer immediately — caught early, jewelry adjustments can sometimes save a migrating piercing.
Keloids and Hypertrophic Scarring
Keloids are raised scar tissue that grows beyond the boundary of the original wound, distinct from hypertrophic scars, which stay within the wound’s borders. The genetic component is significant and worth knowing about before you book a snug.
The primary risk factor for keloids is darkly pigmented skin, which carries a 15- to 20-fold increased risk, with familial predisposition recognized as autosomal dominant or recessive. Black, Hispanic, and Asian persons are far more likely to develop keloids than white persons, and keloids are more common in persons younger than 30, with risk peaking between ages 10 and 20. In the United States, keloids occur in about 1 in 30 Black individuals, approximately a 20-fold increase in risk compared with White individuals.
If you have a personal or close family history of keloid scarring — especially from prior piercings, acne, or surgery — the snug is a higher-stakes piercing for you, and that is worth a real conversation with your piercer and possibly a dermatologist before proceeding. Pressure earrings and silicone sheeting started early can help prevent escalation if a keloid begins forming, but prevention is much easier than treatment.
The bumps people most commonly see at the entry or exit of a snug are usually hypertrophic scars or irritation bumps, not keloids. These respond to addressing the underlying cause — usually a too-tight or too-loose bar, snagging, sleeping pressure, or cheap jewelry — and are not permanent, unlike a keloid.
Snug Piercing Jewelry: Get This Right or the Piercing Won’t Heal
Jewelry choice is not cosmetic — for a snug, it is the single biggest variable you control in healing outcomes after anatomy.
Initial Jewelry
The standard initial piece for a snug is a curved barbell, sized to accommodate swelling. A straight barbell will not follow the natural curve of the anti-helix and will exert constant pressure on the channel; rings and hoops are inappropriate for an unhealed snug piercing because they apply rotational and lateral forces that the cartilage cannot tolerate while healing.
Gauge: 16G is the standard. Some piercers use 14G for added stability when anatomy allows, but 18G is too thin and increases the risk of rejection.
Length: Long enough to leave several millimeters of clearance on each side for swelling, with the understanding that you will downsize to a shorter, snugger fit at 6–12 weeks.
Material — This Is Not Negotiable
The APP recommends specific materials for fresh piercings, and for a piercing as fussy as the snug, generic “surgical steel” is not adequate. The APP suggests implant-certified titanium (Ti6Al4V ELI) that is ASTM F-136 compliant, ASTM F1295, or ISO 5832-3 compliant, or commercially pure titanium that is ASTM F-67 compliant.
Why this matters: ASTM F136 titanium is the same alloy used for surgical implants — Titanium-6Aluminum-4Vanadium ELI (Extra Low Interstitial). The F136 specification lays out the chemical and mechanical requirements to ensure it is safe for long-term wear inside the body, and it is essentially nickel-free, which removes one of the most common drivers of allergic contact dermatitis around piercings.
By contrast, 316L surgical steel contains 8–14% nickel, and “hypoallergenic” labels on surgical steel jewelry are not regulated and can be misleading. For a healed snug, well-made 316L is generally fine; for a fresh one, it is a gamble that is not worth taking.
Solid 14k or 18k gold (nickel-free, alloy-disclosed) is also acceptable for fresh piercings and is sometimes preferred for clients who want a warmer color than titanium provides. Avoid gold-plated and gold-filled jewelry for a fresh, snug fit — the underlying base metal will eventually come into contact with the channel.
Healed Jewelry Snug Piercing Options
Once your snug piercing is fully healed (and only then), styling opens up:
- Curved barbells with decorative ends — gemstones, opals, clusters. The most common long-term choice.
- Small hoops or seamless rings — possible only if your anatomy and healed channel allow; many snugs cannot accommodate a ring at all.
- Clickers — for established piercings with enough channel depth to support the hinge mechanism.
Bar length post-downsize is typically 6–8mm, and getting this right matters: too long and the jewelry catches on hair and pillowcases, accelerating wear and rejection; too short and the ends embed into the cartilage during any swelling event.
Snug Piercing Cost
Pricing for a snug piercing varies by location, studio reputation, and jewelry quality. In the U.S., the piercing service alone typically runs $40–$80, with jewelry charged separately at $40–$150+ for quality implant-grade titanium and significantly more for solid gold. A complete first session at a reputable studio realistically lands in the $80–$200 range. Studios charging notably less are usually using sub-spec jewelry, and for a piercing this difficult, that is the wrong place to economize.
UK and EU pricing typically runs £50–£90 for the service, with jewelry on top.
Choosing a Piercer for a Snug
For a piercing this anatomy-dependent and complication-prone, the piercer matters more than for almost any other ear piercing. Look for:
- APP membership (in the U.S./Canada) or equivalent regional credentialing, such as UKAPP or Australasian United Professional Piercers.
- A portfolio of healed snugs, not just fresh ones. Anyone can produce a fresh piercing that looks good day-of; the test is whether their snugs look good a year later.
- Willingness to turn you down. A piercer who says, “Your anatomy isn’t right for this — let me show you a faux snug instead,” is doing the right thing. Treat that conversation as a signal of competence, not a setback.
- Implant-grade jewelry on hand with mill certificates available on request.
- A studio using single-use, sterile needles — never piercing guns, which are not capable of being properly sterilized and which crush rather than cleanly puncture cartilage.
Bottom Line
A snug piercing is a genuinely beautiful piece, but it is also among the most demanding ear piercings to get and to heal. It depends almost entirely on whether your anti-helix anatomy supports it, on the piercer’s skill in placement, on jewelry that meets ASTM F136 implant-grade standards, and on disciplined aftercare for a full year.
When all of those line up, a healed snug piercing is one of the most distinctive piercings in a curated ear. When any one of them is off — wrong anatomy, gun piercing, cheap steel, sleeping on it nightly — the snug becomes one of the most likely cartilage piercings to reject, scar, or trigger perichondritis. Go in informed, choose a piercer who will be honest with you, and accept that “rushing” this piercing is the fastest way to lose it.
References
- Association of Professional Piercers. Suggested Aftercare for Body Piercings. https://safepiercing.org/aftercare/
- Association of Professional Piercers. Jewelry for Initial Piercings. https://safepiercing.org/jewelry-for-initial-piercings/
- Ziegler, A., et al. Ear Piercing Complications: Comparing Cartilage and Soft Tissue Piercings in a Large Survey Cohort. The Laryngoscope. https://onlinelibrary.wiley.com/doi/10.1002/lary.70572
- Simplot, T.C., Hoffman, H.T. Comparison between cartilage and soft tissue ear piercing complications. American Journal of Otolaryngology, 1998. https://pubmed.ncbi.nlm.nih.gov/9758178/
- Sosin, M., et al. Transcartilaginous ear piercing and infectious complications: a systematic review and critical analysis of outcomes. The Laryngoscope, 2015. https://pubmed.ncbi.nlm.nih.gov/25825232/
- Fisher, C.G., Kacica, M.A., Bennett, N.M. Risk factors for cartilage infections of the ear. American Journal of Preventive Medicine, 2005. https://pubmed.ncbi.nlm.nih.gov/16168869/
- Sismanis, A., et al. Post-piercing perichondritis. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9445946/
- Rajabi-Estarabadi, A., et al. Hypertrophic Scarring Keloids. StatPearls, NCBI Bookshelf. https://www.ncbi.nlm.nih.gov/books/NBK537058/
- Juckett, G., Hartman-Adams, H. Management of Keloids and Hypertrophic Scars. American Family Physician, 2009. https://www.aafp.org/pubs/afp/issues/2009/0801/p253.html
- Multi-ancestry meta-analysis of keloids uncovers novel susceptibility loci in diverse populations. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12368108/
- Rajput, A., et al. Evaluating ear cartilage piercing practices in London, UK. The Journal of Laryngology & Otology, 2014. https://pubmed.ncbi.nlm.nih.gov/24909453/
- American Academy of Dermatology. Caring for Pierced Ears. https://www.aad.org/public/everyday-care/skin-care-basics/tattoos/caring-for-pierced-ears