Rook Piercing Quick Facts
| Detail | Information |
|---|---|
| Placement | Inferior crus of the antihelix (inner ear cartilage ridge above the tragus) |
| Pain level | 6–8 out of 10 |
| Healing time | 9 to 12 months (some take up to 18) |
| Initial jewelry | Curved barbell, 16 gauge, 5/16″–3/8″ length |
| Best jewelry materials | Implant-grade titanium (ASTM F-136 or F-67), 14k+ solid gold, niobium |
| Average cost | $40–$80 for the piercing, $30–$80 for starter jewelry |
| Originated by | Erik Dakota, early 1990s, first printed in Body Play magazine, 1992 |
| Anatomy-dependent? | Yes — not every ear can support it |
| Risk level | Higher than lobe piercings; cartilage infections can be serious |
What Is a Rook Piercing?

A rook piercing passes through the inferior crus of the antihelix, the small ridge of cartilage that sits between the triangular fossa and the conch on the inner ear. Unlike most ear piercings that span a front-to-back surface, the rook goes vertically through a fold, so the jewelry rests perpendicular to the side of the head.
It sits directly above the daith and below the upper helix curve. The rook piercing is anatomy-dependent: the ridge has to be pronounced enough to hold jewelry without compressing against itself.
Anatomy and Why It Decides Everything
The auricle is built from a thin sheet of elastic cartilage covered by skin that adheres tightly to the perichondrium. According to a clinical review of post-piercing perichondritis published on PubMed Central (PMC9445946), cartilage nutrition is carried out by the contiguous perichondrium, which must remain adhered to the cartilage to avoid necrosis. The antihelix has no independent blood supply.
That single anatomical fact explains nearly everything about the rook: why some ears can’t take it, why it hurts more than a helix, why healing takes close to a year, and why curved barbells almost always beat hoops in the early months.
The rook piercing was originated and named by professional piercer Erik Dakota, and it first appeared in print in issue #4 of Body Play and Modern Primitives Quarterly in 1992, making it younger than many working piercers today.
Not Every Ear Has a Rook Piercing
The antihelix has to be pronounced, deep, and thick enough to hold a piece of jewelry without the cartilage being squeezed against itself. If the ridge is shallow, flat, or splits in an unusual way, an honest piercer will turn the appointment down or suggest a snug or vertical rook variation instead.
Signs your anatomy is not suited:
- The antihelix ridge sits flush with the surrounding cartilage rather than rising above it
- The fold is so tight that no jewelry can sit between the inner and outer wall without pressure
- The ridge angles sharply upward or splits into two crura with no clear single pierceable spot
Forcing a rook through unsuitable anatomy is the most common reason these piercings reject, migrate, or refuse to heal even after a year.
Rook Piercing Pain
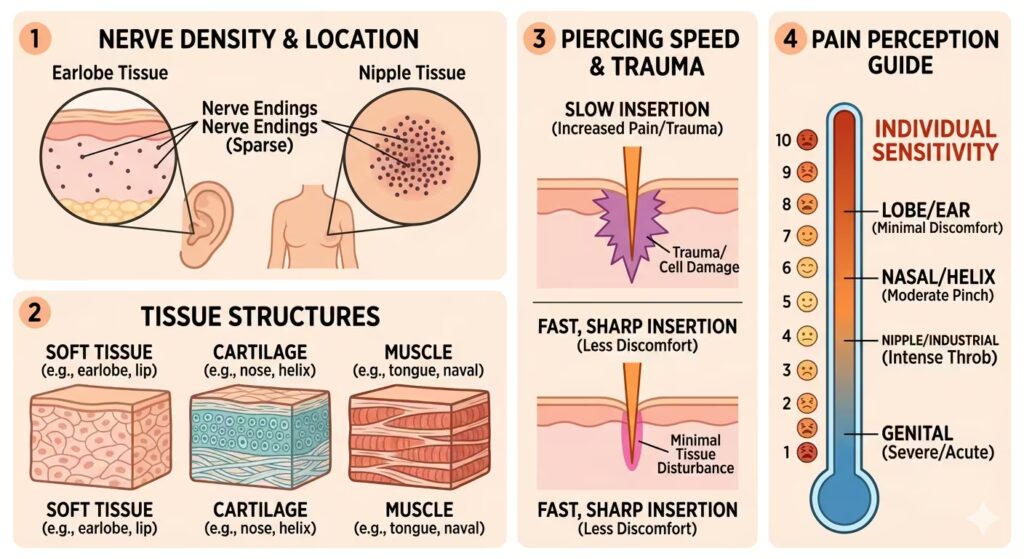
People rate the rook between 6 and 8 out of 10, higher than a helix and comparable to or slightly above a daith. Three reasons explain this:
- The antihelix cartilage in this region is denser than the helix or earlobe, so the needle meets more resistance.
- Many people report the audible cartilage crunch as more disturbing than the actual pain.
- Because the needle travels through a fold rather than a single surface, the sensation lasts longer than a typical perforation.
A 2025 review on post-piercing inflammation, published in PMC (PMC12110840), notes that piercing introduces mechanical trauma that disrupts tissue integrity, leading to localized swelling, redness, and pain. The intensity varies based on body site, individual sensitivity, technique, and aftercare.
The pain itself lasts two to three seconds. The lingering soreness peaks in the first one to two weeks, then tapers over the first two months.
Rook Piercing Healing
Cartilage piercings heal from the outside surface inward. The skin closes over while the internal channel is still forming, which means the piercing can look healed long before it actually is.
For the rook specifically, plan on 9 to 12 months, with some people taking up to 18. Three factors slow the process:
- Auricular cartilage is avascular. Healing depends entirely on diffusion from the perichondrium and surrounding skin.
- The rook sits at the convergence of the forward helix, conch, and tragus. Phones, headphones, pillows, and hair brushing all transmit pressure to it.
- The rook tucks behind the helix flap, so most people can’t see their own piercing in a single mirror. Crusting and debris accumulate in places that go unnoticed.
A 2014 study in the Journal of Laryngology and Otology evaluating ear cartilage piercing practices in London (PubMed 24909453) found that while 96% of practitioners were aware of the risk of infection post-piercing, only 4% were aware of keloid scarring, 12% of hypertrophic scarring, and 0% of cauliflower ear. The people performing the piercing are often less informed about long-term complications than the people getting it.
A Realistic Rook Piercing Healing Timeline
- Days 1–7: Sharp throbbing, swelling, redness, and clear or pale yellow crusting. Sleeping on the side is painful or impossible.
- Weeks 2–6: Swelling subsides, but the area stays tender to the touch. The piercing may weep lymph daily.
- Months 2–4: External skin closes over. The fistula through the cartilage is still forming and remains fragile.
- Months 4–9: Soreness fades. Crusting reduces but doesn’t fully stop.
- Months 9–12: Internal channel matures. Jewelry can usually be downsized or changed by a professional.
Do not change the jewelry yourself before the nine-month mark. Cartilage fistulas collapse easily, and once a healing piercing has been forced, another six months can be added to the process.
Rook Piercing Risks
A 1998 study in the American Journal of Otolaryngology (PubMed 9758178) surveying 1,000 nurses found a 30% complication rate for cartilage piercings versus 21% for soft tissue piercings, with minor infection more prevalent in cartilage and allergic reaction more common in soft tissue. That is a significantly higher complication baseline than lobe piercings. Source: https://pubmed.ncbi.nlm.nih.gov/9758178/
Perichondritis and Pseudomonas
The most dangerous rook complication is perichondritis, an infection of the perichondrium and underlying cartilage. A 2015 systematic review in The Laryngoscope analyzing transcartilaginous piercing infections (PubMed 25825232) concluded that transcartilaginous post-piercing infection may lead to ear deformity and hospitalization, and that Pseudomonas is the most common bacterial cause. Source: https://pubmed.ncbi.nlm.nih.gov/25825232/
A 2004 outbreak investigation by Oregon public health agencies, published in JAMA (PubMed 14982914), traced Pseudomonas aeruginosa infections directly to commercial upper-ear cartilage piercing. The study concluded that ear cartilage piercing is inherently more risky than lobe piercing, and that clinicians should respond aggressively to potential auricular chondritis and consider Pseudomonas a likely cause pending culture results. Several confirmed cases required surgical drainage. Several were left with permanent cosmetic deformity.
A separate case-control study in the American Journal of Preventive Medicine (PubMed 16168869) on a 2003 outbreak of auricular chondritis identified contaminated aftercare solution as a key risk factor. 60% of confirmed cases required hospitalization for a median of 4.4 days and treatment with intravenous and oral antibiotics.
What this means in practice:
- Choose a studio that uses sealed, single-use sterile saline rather than bulk solution from a sprayed bottle.
- Watch for redness that spreads beyond the piercing site, persistent throbbing pain after week three, fever, or any drainage with a foul smell. These are signs to see a doctor, not to wait it out.
- Cartilage infections progress more rapidly than lobe infections and can permanently deform the ear.
Cauliflower Ear From a Piercing Is Real
Untreated perichondritis can lead to subperichondral abscess, cartilage necrosis, and the cosmetic deformity known as cauliflower ear. Once cartilage loses its perichondrial blood supply, it dies and collapses. Reconstructive surgery rarely restores the original shape.
Bumps, Migration, and Rejection
Beyond infection, rook piercing is prone to three lower-stakes but more common issues:
- Hypertrophic bumps. Raised, firm bumps from trauma or pressure. Almost always caused by sleeping on the piercing, snagging, or wearing tight headphones.
- Migration. The jewelry slowly moves toward the skin’s surface. Usually caused by jewelry that’s the wrong shape (a CBR instead of a curved barbell early on) or wrong length.
- Rejection. The body pushes the piercing out entirely. The rook has a relatively low rejection rate compared to surface piercings because cartilage anchors the jewelry on both sides; however, rejection still occurs when the antihelix is not pronounced enough or when poor jewelry design causes chronic irritation.
A 2008 histologic study in the Journal of Plastic, Reconstructive and Aesthetic Surgery (PubMed 17684004) found that all piercing methods cause the same extent of damage to cartilage and perichondrium. Prevention of perichondritis depends on hygiene and aftercare rather than technique. An expensive studio with good sterile practice matters far more than which specific piercing tool the piercer prefers.
The Piercing Gun
The Association of Professional Piercers states that piercing guns are never appropriate for any piercing, including earlobes. Spring-loaded guns cannot be properly sterilized, fire blunt studs through cartilage by force rather than cutting, and crush surrounding tissue. Every documented serious cartilage infection outbreak in the medical literature involves either a gun or contaminated aftercare. A real rook is done with a hollow needle, single-use, by a piercer wearing fresh gloves.
Rook Piercing Jewelry
The Association of Professional Piercers’ Minimum Standards for jewelry in initial piercings is the most authoritative reference. For initial piercings, the APP requires:
- Implant-certified titanium that is ASTM F-136 compliant, ASTM F1295, or ISO 5832-3 compliant, or commercially pure titanium that is ASTM F-67 compliant
- Surgical steel that is ASTM F-138 or ISO 5832-1 compliant
- Solid 14k or higher nickel- and cadmium-free gold
- Niobium
- Platinum
What is not on that list: sterling silver, gold-plated, gold-filled, gold vermeil, “surgical steel” without a grade designation, or anything labeled hypoallergenic without certification. According to the FDA, the term hypoallergenic has no federal standard and means whatever a manufacturer wants it to mean. The same is largely true of generic “surgical steel.”
Best Initial Jewelry
A curved barbell at 16 gauge is the consensus starter jewelry for a rook piercing. The reasoning:
- A curved barbell follows the natural arc of the antihelix fold and doesn’t put outward pressure on the healing channel the way a captive bead ring does.
- 16 gauge (1.2 mm) is thick enough to support the cartilage and resist tearing, but thin enough that the piercing itself is not unnecessarily traumatic.
- A length of 5/16″ (8 mm) to 3/8″ (10 mm) is standard, with a built-in swelling room. The piercer downsizes this once the initial swelling resolves at the 2–3 month mark.
Hoops, captive bead rings, and clickers can look stunning in a rook, but the increased curvature of a small-diameter ring presses against both walls of the fistula and slows healing or causes migration. Save them for after the nine-month mark.
Materials
- Implant-grade titanium (ASTM F-136 or F-67). The standard for fresh piercings. Lightweight, inert, and anodizable into a range of colors without coating. Ideal for anyone with nickel sensitivity.
- 14k or 18k solid gold. Beautiful and biocompatible if it’s nickel-free and cadmium-free. Avoid gold above 18k for body jewelry because it’s too soft and dents easily. Never gold-plated, gold-filled, or vermeil for a fresh piercing — the thin gold layer wears off and exposes a base metal that may cause a reaction.
- Niobium. Hypoallergenic, anodizable, and less commonly used, but excellent for those who react even to titanium.
- Implant-grade steel (ASTM F-138). Acceptable, but contains 10–14% nickel. Choose titanium if nickel reactivity is a concern.
Rook Piercing Aftercare
The aftercare guidance for rook piercing that the APP, dermatologists, and current medical literature agree on is:
What to Do
- Sterile saline, twice daily. A sterile 0.9% sodium chloride wound wash spray (such as NeilMed Piercing Aftercare or Wound Wash Saline) is applied in the morning and evening. Spray directly onto the piercing, let it sit for 30 seconds, then pat dry with a clean disposable paper product.
- Wash your hands before any contact. Don’t touch the piercing otherwise.
- Sleep on the opposite side. A travel pillow or piercing donut pillow takes pressure off the neck through the night, which is the single biggest cause of bumps.
- Stay out of pools, hot tubs, lakes, and oceans for at least the first 4–6 weeks. Open water carries Pseudomonas, the same bacterium responsible for the cartilage infections documented in the JAMA outbreak study.
What Not to Do
- No alcohol, hydrogen peroxide, Bactine, or rubbing alcohol. All of these kill the new cells the body uses to heal.
- No Neosporin or antibiotic ointments. They seal off oxygen and trap bacteria around the piercing.
- No homemade salt soaks. Mixing your own sea salt solution is almost always too concentrated, which dries the piercing and slows healing.
- No tea tree oil, vitamin E, aspirin paste, or “bump treatments.” None are evidence-based for piercing aftercare and most cause the irritation that creates bumps.
- No twisting, rotating, or moving the jewelry. This was 1990s advice that has been thoroughly discredited.
- No earbuds or over-ear headphones for the first 2–3 months. Both transmit constant pressure and harbor bacteria.
When Something Is Wrong
Normal: clear or pale yellow crusting, mild redness, soreness for the first 2–6 weeks, occasional flares from a snag.
Not normal — see a piercer or doctor:
- Spreading redness extending more than a centimeter beyond the piercing
- Hot, throbbing pain that intensifies after the third week instead of fading
- Yellow-green or foul-smelling discharge
- Fever
- A hard lump that grows rather than shrinks over weeks
The 2015 Laryngoscope systematic review found that a delay in presentation was associated with worse outcomes in cartilage-piercing infections. If something feels seriously wrong, act early.
The Migraine Question
Many people consider a rook (or its neighbor, the daith), hoping for migraine relief. Based on current peer-reviewed research, there is no clinical trial evidence that rook or daith piercings treat migraines.
A 2024 narrative review in Headache: The Journal of Head and Face Pain searched the literature for evidence on daith piercing and migraine. From 186 identified articles, only one retrospective study and three case reports met the inclusion criteria. No clinical trials were identified.
A 2017 case report in Frontiers in Neurology (PMC5711775) proposed a possible mechanism — stimulation of vagal afferents in the ear — but the authors concluded that daith piercing cannot be recommended as migraine treatment because of the lack of scientific evidence, the unquantified rate of failure, and the associated risks with insertion.
The American Migraine Foundation states that the risks of a daith piercing outweigh the reward, that the results are attributable to the placebo effect, and that the piercing carries a high risk of infection. The Cleveland Clinic position is the same: no evidence supports the claim that daith piercings relieve migraine. Source:
Survey data from the London Migraine Clinic and MigrainePal report initial improvement in roughly 47% of respondents, but these are self-selected, uncontrolled, and subject to placebo and recall bias. As of 2026, no randomized controlled trial has been published for either piercing.
If migraine relief is the only reason for considering a procedure, evidence-based treatments are the better path: triptans, CGRP inhibitors, non-invasive vagus nerve stimulation, preventive medications, or auricular acupuncture. Get a rook for the look, not as a treatment.
Rook Piercing Cost
A rook piercing from a reputable APP-member studio runs $40–$80 for the piercing service alone. Quality implant-grade titanium starter jewelry adds another $30–$80, and gold pieces go higher. Total cost for a rook done properly: $70–$200.
Mall kiosks and beauty supply stores often offer cheaper rates, sometimes using piercing guns. Every documented serious cartilage infection outbreak in the medical literature involves either a gun, untrained staff, or contaminated aftercare solution. The savings are not worth the risk of perichondritis or cauliflower ear.
How to Choose a Piercer
- Verify APP membership at safepiercing.org. Membership requires demonstrated training, specific equipment, and adherence to jewelry and aftercare standards.
- Ask to see jewelry mill certificates. Reputable studios have ASTM/ISO certification documents from their jewelry suppliers and will show them.
- Confirm needle and single-use sterile technique. No gun, no reused jewelry, fresh gloves, autoclave-sterilized tools.
- Ask the piercer to assess the anatomy honestly. A piercer who agrees to do a rook on every walk-in, regardless of ear shape, is a piercer who produces rejected piercings. The right answer for some ears is “I don’t recommend it.”
- Look at healed work. Healed photos at six and twelve months show more than freshly done photos.
Changing Jewelry, Stretching, and Adding More Piercings
- First downsize: 8–12 weeks, done by a piercer to switch the longer initial barbell for one fitted to settled anatomy.
- First aesthetic change: not before 9 months, ideally 12. The first change should be done by a piercer.
- Stretching: the rook is rarely stretched. The cartilage anchor is not flexible enough to accommodate gauging in most cases.
- Adding more piercings nearby: wait until the rook is fully healed. Multiple cartilage piercings in close proximity dramatically slow each other’s healing.
Rook Piercing Frequently Asked Questions
Does a rook piercing hurt more than a daith?
Slightly. The rook piercing passes through denser cartilage in the antihelix, while the daith passes through the helix root. Most people rate the rook at 6–8 and the daith at 5–7.
Can I sleep on my rook piercing?
Not for the first 4–6 months, and ideally not at all during the first year. A donut-shaped travel pillow is the best solution for side sleepers.
Why does my rook piercing still hurt after six months?
Persistent soreness past six months usually points to one of three causes: poor jewelry fit (often a barbell that’s too long now that swelling has gone down), sleeping on the side, or anatomy that’s not quite right for a stable rook. Have a piercer assess it.
Can I wear earbuds or headphones with a rook piercing?
Earbuds should be avoided for at least the first 2–3 months. Over-ear headphones are slightly safer but still press on the area and harbor bacteria. After healing, both are fine.
What if my rook bumps appear?
Most “rook bumps” are hypertrophic scars caused by physical trauma — sleeping on it, snagging it, or wearing the wrong jewelry. Don’t apply tea tree oil, crushed aspirin, or chamomile compresses. Remove the source of trauma, switch to a properly fitted curved barbell in implant-grade titanium, and let the bump shrink on its own.
Can I get a rook piercing on both ears at once?
Sleeping is the obstacle. With both ears pierced, side-sleeping on either side puts pressure on a healing rook piercing. Most piercers recommend doing one at a time, with at least six months between them.
How long until I can change the jewelry myself?
A full year minimum. The first change should be made by a piercer, and subsequent changes are easier if the jewelry has an internally threaded or threadless design. Forcing a threaded post through a rook fistula damages the channel.
Is the rook piercing the same as a snug piercing?
No. The snug sits on the antihelix as well, but on the outer cartilage ridge that runs along the side of the ear, visible from the front. The rook piercing sits on the inner ridge tucked behind the forward helix.
Can I take a rook out and let it close?
Yes, but cartilage closure leaves a small indent or scar where the fistula formed. A fully healed rook closes from the inside but rarely vanishes completely on the surface.
Will an MRI affect my rook jewelry?
Implant-grade titanium and niobium are MRI-safe. Steel jewelry is generally safe in modern MRI machines, but it should be disclosed to the technician. Plated or unmarked jewelry should be removed if possible.
Sources
- Association of Professional Piercers, Minimum Standards for Jewelry for Initial Piercings: https://safepiercing.org/jewelry-for-initial-piercings/
- American Migraine Foundation, Daith Piercings as Migraine Treatment: https://americanmigrainefoundation.org/resource-library/daith-piercings-101/
- Simplot TC, Hoffman HT. Comparison between cartilage and soft tissue ear piercing complications. American Journal of Otolaryngology, 1998: https://pubmed.ncbi.nlm.nih.gov/9758178/
- Sosin M, et al. Transcartilaginous ear piercing and infectious complications: a systematic review. The Laryngoscope, 2015: https://pubmed.ncbi.nlm.nih.gov/25825232/
- Keene WE, et al. Outbreak of Pseudomonas aeruginosa infections caused by commercial piercing of upper ear cartilage. JAMA, 2004: https://pubmed.ncbi.nlm.nih.gov/14982914/
- Fisher CG, Kacica MA, Bennett NM. Risk factors for cartilage infections of the ear. American Journal of Preventive Medicine, 2005: https://pubmed.ncbi.nlm.nih.gov/16168869/
- Mandavia R, et al. Evaluating ear cartilage piercing practices in London, UK. Journal of Laryngology and Otology, 2014: https://pubmed.ncbi.nlm.nih.gov/24909453/
- van Wijk MP, et al. Ear piercing techniques and their effect on cartilage, a histologic study. Journal of Plastic, Reconstructive and Aesthetic Surgery, 2008: https://pubmed.ncbi.nlm.nih.gov/17684004/
- Soares VYR, et al. Post-piercing perichondritis: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9445946/
- Pradhan A, et al. Daith piercing: Revisited from the perspective of auricular acupuncture systems. A narrative review. Headache, 2024: https://headachejournal.onlinelibrary.wiley.com/doi/abs/10.1111/head.14672
- D’Amico D, et al. Daith Piercing in a Case of Chronic Migraine: A Possible Vagal Modulation. Frontiers in Neurology, 2017: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5711775/
- Novel Gels for Post-Piercing Care: Evaluating Pranoprofen Formulations, PMC: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12110840/